
Do GLP-1 Drugs Cause Muscle Loss? What Patients Should Know Before Starting Ozempic, Wegovy, or Zepbound

In the STEP 1 trial of semaglutide, the drug that became Wegovy, patients lost an average of 15% of their body weight over 68 weeks. About 39% of that loss came from lean tissue rather than fat. That number has fueled a wave of concern about "muscle loss" on Ozempic, Wegovy, and Zepbound.
But lean tissue is not the same as skeletal muscle. It also includes water, organs, bone, and connective tissue, and most of what's lost during weight reduction tracks proportionally with the body getting smaller.
In the same trial, relative lean mass actually went up. Whether a patient holds onto skeletal muscle and strength depends less on the drug itself and more on protein intake, resistance training, and how fast the weight comes off.
This article is for educational purposes only and does not replace medical advice. Do not start, stop, or change a prescription medication without speaking with a licensed clinician.
Key Takeaways
About a quarter to a third of weight lost on GLP-1 drugs is lean tissue, but only part of that is skeletal muscle. The rest is water, organs, bone, and connective tissue.
Real-world data suggests muscle loss is often modest. In one 2026 cohort of 486 patients, skeletal muscle dropped about 5% while fat dropped roughly 18%.
The two interventions with the strongest evidence for protecting muscle are resistance training and eating enough protein. Walking helps the heart but does little for muscle.
Risk is higher for older adults, postmenopausal women, anyone losing weight quickly, and patients who get hit hard by nausea or early fullness.
Track strength, not just the scale. Grip, stair-climb, and the ability to stand from a chair five times tell you more than a number on a DEXA report.
Don't stop Ozempic, Wegovy, or Zepbound on your own.
Review MedicalResearch.com’s guide to theOzempic dosing schedule before your next appointment.
Do GLP-1 Drugs Cause Muscle Loss?
Not directly. GLP-1 receptor agonists (semaglutide in Ozempic and Wegovy, and the dual GIP/GLP-1 agonist tirzepatide in Zepbound) work by suppressing appetite and slowing how fast the stomach empties. Patients eat less, often substantially less, and the weight comes off. In trials, that's averaged anywhere from 5% to 18% of body weight depending on the drug and dose.
What these drugs don't do is attack muscle tissue. The lean mass that gets lost during treatment is lost the same way it would be after bariatric surgery or on a very-low-calorie diet: when the body shrinks, every tissue shrinks with it, muscle included. The useful question isn't whether some lean tissue is lost. It almost always is. The question is whether skeletal muscle and functional strength hold up, and that depends largely on what the patient does during treatment.
What Is Lean Mass, and Is It the Same as Muscle?
No, and the difference matters more than most headlines admit. When a study reports that someone lost 5 kg of lean mass, that doesn't mean they lost 5 kg of muscle. Lean mass is a wide category that includes everything in the body that isn't fat.
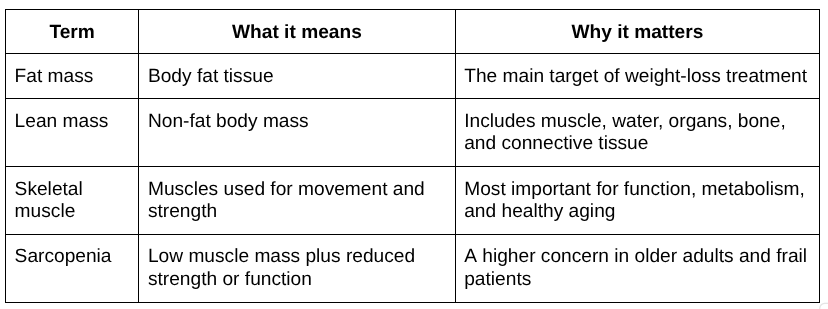
Skeletal muscle is roughly half of total lean body mass in most adults. So when the STEP 1 trial reported 39% of weight loss coming from lean mass, the actual skeletal muscle component was closer to 20% of total weight lost. The rest was water, organ tissue, connective tissue, and bone.
This is why body-composition scans like DEXA and bioelectrical impedance, while useful, only tell part of the story. Hydration alone can shift lean mass readings by a kilogram or more from one week to the next. What better predicts whether someone has lost muscle that matters is whether their grip is weaker, whether stairs feel harder, or whether they can still stand up from a low chair without using their hands.
How Much Lean Mass Can People Lose on GLP-1 Medications?
The honest answer is that it varies, but the body-composition data from the major trials cluster within a fairly predictable range.
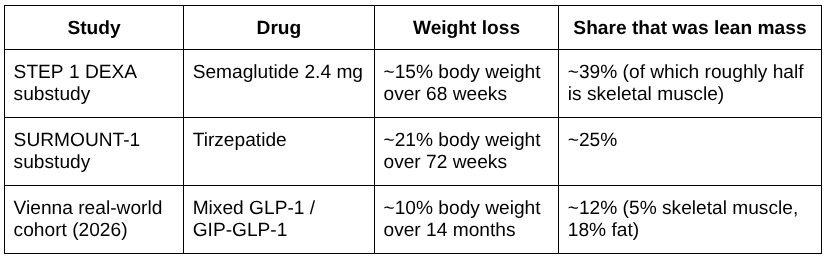
A few things stand out across the data. The STEP 1 lean mass figure looks high until you remember that lean mass includes water and organs. When the researchers separated out skeletal muscle, the proportion of muscle to body weight actually went up, and the lean-to-fat ratio improved most in patients who lost the most weight.
In SURMOUNT-1, about three-quarters of the weight tirzepatide patients lost was fat, in line with what bariatric surgery typically produces. An MRI substudy of patients with type 2 diabetes on tirzepatide found that muscle fat infiltration decreased, meaning the remaining muscle got cleaner, not just smaller.
The Vienna cohort is the most informative for real-world expectations because it tracked patients who got general exercise advice rather than structured trial protocols, and most of them kept their muscle mass. More than 70% of those patients preserved or increased their relative skeletal muscle.
The pattern across all three: fat loss dominates, lean mass drops in proportion, and skeletal muscle loss is usually a smaller slice than the headline lean-mass number suggests.
Why Can Weight Loss Lead to Muscle Loss?
Muscle is use-it-or-lose-it tissue. When the body is in a calorie deficit and isn't getting enough protein or being asked to do anything physically demanding, it sees no reason to keep muscle it isn't using. A few mechanisms compound this on GLP-1 drugs in particular.
The first is simple math. Appetite suppression is the main reason these medications work — patients eat 16% to 39% fewer calories on average, according to trial data. When protein intake drops along with everything else, the body runs short on the amino acids it needs for muscle repair. Nausea, vomiting, and the feeling of being full after a few bites can push intake even lower in the first weeks of treatment.
The second is hormonal. Insulin and IGF-1, both anabolic signals that tell muscle to grow and repair, fall during sustained weight loss. Lower insulin is generally a good thing for metabolic health, but it also means less of the signaling that maintains muscle protein synthesis.
The third is behavioral. Many patients move less during the early months of GLP-1 treatment, often because of fatigue or reduced food intake. Without mechanical loading from resistance work, muscle has no reason to stick around. This is the mechanism patients can most directly control.
If you are researching gut-support options, MedicalResearch.com also explainsLactobacillus rhamnosus and what patients should know about this probiotic strain.
Who Is Most at Risk for Muscle Loss on GLP-1 Drugs?
The risk isn't evenly distributed. A 70-year-old postmenopausal woman with type 2 diabetes losing weight quickly on tirzepatide faces a very different muscle-preservation challenge than a 35-year-old man on the same drug. The groups below have meaningfully higher baseline risk, roughly ranked by clinical concern.
Older adults, especially over 65. Sarcopenia prevalence climbs sharply after 60, and the body becomes resistant to the muscle-building signal from protein and exercise (anabolic resistance). Weight loss in this group can convert latent muscle weakness into measurable functional decline.
Postmenopausal women. Falling estrogen accelerates both muscle and bone loss independent of weight changes. Layering rapid weight loss on top of that compounds the risk in a way premenopausal women don't typically face.
Patients with type 2 diabetes. Baseline sarcopenia is already elevated in T2D, with prevalence estimates ranging from 7% to 29% depending on diagnostic criteria. This is the group most clinical guidance explicitly flags for body-composition monitoring.
Anyone losing weight rapidly. When weight comes off faster than about 1% of body weight per week sustained over months, lean-mass preservation gets harder regardless of age. The Joint Advisory specifically notes that weight loss of 14% or more over three to four months is associated with significant bone loss as well.
Patients with persistent GI side effects. Nausea, vomiting, or severe early satiety that lasts beyond the first few weeks of treatment means intake is chronically too low, which is when protein deficits become a real problem.
Sedentary patients and anyone already frail. Without a resistance stimulus, the body has no reason to defend muscle during weight loss. For frail patients, even a modest strength drop can affect the ability to live independently.
If a patient falls into one of the top three groups, the conversation about muscle preservation should happen before the first injection, not after weakness shows up.
How Can Patients Protect Muscle While Taking Ozempic, Wegovy, or Zepbound?
What actually works falls into two categories: the things every patient should do, and the things some patients should add. Here's the practical layer.
The two that matter most.
Resistance training and protein intake do the bulk of the work. Skip either one and the rest of this list barely helps. Walking is fine for cardiovascular health, but it does almost nothing for muscle preservation. You need to load the muscle to keep it. Two to three sessions a week of weights, bands, machines, or bodyweight exercise is the floor.
On the protein side, aim for adequate intake spread across meals rather than one big protein-heavy dinner, because muscle protein synthesis has a per-meal ceiling around 20 to 25 grams in most adults.
Don't stack a crash diet on top of the medication.
GLP-1 drugs already cut calorie intake by 16% to 39% on average. Adding an aggressive low-calorie diet on top of that accelerates lean mass loss with no real benefit, because the medication is already doing the work. If weight is coming off too fast (more than about 1% of body weight per week sustained over months) that's a conversation to have with the prescribing clinician.
Treat GI side effects as a nutrition problem.
Nausea, vomiting, and severe early satiety aren't just uncomfortable. They cut protein and calorie intake at the exact moment muscle preservation is hardest. Anti-nausea medication, smaller and more frequent meals, and slower dose escalation are all reasonable strategies to discuss before symptoms drive intake into the ground.
Track strength, not just the scale.
Three home tests are worth knowing:
How long it takes to stand from a chair five times without using your hands,
How many flights of stairs you can climb without stopping,
Grip strength if you have access to a dynamometer.
If any of these get noticeably worse during treatment, that's a signal worth bringing to a clinician.
Get a baseline body-composition reading if you can.
A DEXA scan before starting treatment gives you something to compare against later. It's especially worth doing for patients over 60 or anyone already in one of the higher-risk groups. Bioelectrical impedance from a clinic or even a good home scale is a workable substitute when DEXA isn't accessible.
For patients who can access one, a registered dietitian with experience in weight management is the single most useful person to add to the care team. They can build a protein and meal-timing plan around the appetite reduction, which is more practical than trying to figure it out alone.
For a broader foundation, read MedicalResearch.com’s guide toholistic health lifestyle changes.
How Much Protein Do Patients Need on GLP-1 Medications?
The honest answer depends on the patient, but the range most clinicians work with is 1.2 to 1.6 grams of protein per kilogram of adjusted body weight per day during active weight loss. That's the figure the joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society points to, with a floor of roughly 0.4 to 0.5 g/kg/day below which muscle starts to suffer measurably.
For a 90 kg adult, that lands somewhere between 108 and 144 grams of protein per day. For a 70 kg adult, between 84 and 112. These are starting points. Older adults, very active patients, and people doing serious resistance training tend to sit at the higher end of the range. Patients with kidney disease should not assume the upper end is safe and need to set a target with their nephrologist or a registered dietitian.
The harder problem on GLP-1 drugs is hitting it when appetite has dropped 30%. A few things help:
Lead with protein at every meal. When you only have room for a small amount of food, the protein should go in first. Eggs, Greek yogurt, cottage cheese, fish, and chicken are nutrient-dense per bite and tend to be well-tolerated even when GI side effects are active. Tofu, beans, and lentils work for plant-based patients but take up more stomach volume per gram of protein.
Use shakes when food won't fit. A 30-gram whey or soy protein shake can rescue a day where solid food isn't appealing. They're not a replacement for real meals long-term, but they're often the difference between hitting a daily protein target and missing it by 40 grams.
Spread it across the day. Muscle protein synthesis caps out around 20 to 25 grams per meal in most adults, so three or four moderate-protein meals do more for muscle than one big dinner. This matters more on GLP-1 drugs because patients tend to skip breakfast naturally as appetite drops.
The single biggest failure mode is eating one small meal a day with minimal protein, hitting the day's target on a scale of zero out of needed, and wondering why strength is dropping after a few months.
Why Resistance Training Matters During GLP-1 Weight Loss
Resistance training is what tells the body to hold onto muscle while everything else gets smaller. Protein alone won't do it. The body has to be loading the muscle hard enough that breaking it down would feel like a bad decision metabolically.
A 2024 randomized trial compared liraglutide alone against liraglutide combined with structured exercise over a year. The exercise group held onto bone mineral density that the medication-only group lost. They also showed bigger drops in visceral fat and inflammatory markers. Both groups lost similar amounts of weight. The difference was what their bodies looked like underneath.
For most patients, two or three sessions a week is enough. The work should hit the legs, back, chest, shoulders, and core somewhere across the week, and it should be hard enough that the last few reps of each set feel difficult. Free weights, machines, bands, bodyweight movements all work fine. Walking doesn't. Aerobic exercise is good for the heart and helps with energy on bad days, but it doesn't preserve muscle.
If a patient has never lifted anything before, paying for four or five sessions with a trainer or physical therapist at the start saves months of wasted effort. The mistake isn't usually injury, it's just spending six months on movements that don't actually challenge the muscle. Patients over 60 or with joint or cardiac issues should get a real plan from their clinician, not just verbal permission to start.
Should Older Adults Be More Cautious?
Yes. Sarcopenia is already doing work in the background after age 60. Roughly 1% of muscle mass disappears per year. Adding a major weight loss event on top can compress years of decline into a few months.
Walking speed is the cleanest thing to track. If it drops more than 0.1 m/s over a few months, that's worth a conversation. Grip strength is useful too and takes under a minute at a clinic visit. The chair-stand test from earlier in this article works at home. Falls, even small ones that don't cause injury, shouldn't be brushed off. They usually mean leg strength is slipping faster than the patient has noticed.
On dosing, some obesity medicine specialists prefer slower titration schedules for patients over 65. This is partly to soften GI side effects and partly to give the body time to adjust.
What Should Patients Ask Their Doctor Before Starting a GLP-1 Drug?
A short list of questions can make initial visits more useful:
Am I at risk for muscle loss or sarcopenia?
What protein target is safe for me, given my kidneys and other conditions?
Should I see a registered dietitian?
What type of exercise is safe for me to start with?
Should I track body composition, waist size, strength, or mobility over time?
What side effects could interfere with eating enough?
How quickly should I expect to lose weight, and what pace is too fast?
Should kidney, liver, or metabolic labs be monitored?
Could this medication interact with my other prescriptions?
What warning signs should make me call the office?
Can Supplements Help Prevent Muscle Loss on GLP-1 Drugs?
Not in any direct way. The intervention that protects skeletal muscle during weight loss is resistance training combined with adequate protein. No pill, powder, or stack does this work, and supplement marketing that implies otherwise is overpromising.
That said, there are reasonable supplemental considerations that come up during GLP-1 treatment, just not for muscle preservation specifically. Vitamin D, calcium, and B12 are commonly flagged in clinical guidance because intake of all three tends to drop when overall food intake drops. A daily multivitamin covers most of that for most patients.
Liver health is the other area patients sometimes ask about, partly because obesity and fatty liver disease are closely linked and partly because rapid weight loss can briefly stress the liver as fat mobilizes. Some patients explore options liketargeted liver health supplements as part of a broader wellness approach during this period.
The short version: Muscle is protected by training and protein. Other supplements may have their place for other reasons, but none of them substitute for the work.
Frequently Asked Questions
Do GLP-1 drugs make you lose muscle or fat?
Most of the weight lost on GLP-1 drugs is fat. In trial data, fat typically accounts for 65 to 75 percent of total weight loss, with the rest coming from lean tissue, which includes water, organs, and connective tissue as well as muscle. Skeletal muscle loss is usually a smaller share than the lean-mass headline suggests.
Is lean mass the same as muscle?
No. Lean mass is everything in the body that isn't fat, including water, organs, bone, connective tissue, and skeletal muscle. Skeletal muscle makes up about half of lean body mass in most adults, so a drop in lean mass is not the same as an equivalent drop in muscle.
Can protein prevent muscle loss on Ozempic or Wegovy?
Protein alone won't prevent muscle loss, but adequate protein is one of the two interventions that matters most. The other is resistance training. Joint guidance suggests 1.2 to 1.6 grams of protein per kilogram of adjusted body weight per day during weight loss, with the exact target set by a clinician or dietitian based on kidney function and other factors.
Is Zepbound more likely to cause muscle loss than Wegovy?
The proportions are similar. Both medications produce weight loss that is roughly 70 to 80 percent fat and 20 to 30 percent lean tissue. Tirzepatide (Zepbound) tends to drive more total weight loss than semaglutide (Wegovy), so the absolute amount of lean mass lost can be higher, but the ratio is comparable.
Should older adults take GLP-1 drugs?
Older adults can benefit from GLP-1 therapy, but they need closer monitoring because age-related muscle loss compounds weight-loss-related muscle loss. Walking speed, grip strength, and the ability to stand from a chair without using the hands are useful markers. Slower dose titration is often appropriate for patients over 65.
Can supplements stop GLP-1 muscle loss?
No. No supplement has been shown to prevent GLP-1-related muscle loss. Muscle is preserved by resistance training and adequate protein intake. Supplements like vitamin D, calcium, or B12 may be useful for general nutrition during reduced food intake, but they don't substitute for training and protein.